Obsessive–compulsive disorder
Obsessive–compulsive disorder
Jump to navigation
Jump to search
| Obsessive–compulsive disorder | |
|---|---|
 | |
| Frequent, excessive hand washing occurs in some people with OCD | |
| Specialty | Psychiatry |
| Symptoms | Feel the need to check things repeatedly, perform certain routines repeatedly, have certain thoughts repeatedly[1] |
| Complications | Tics, anxiety disorder, suicide[2][3] |
| Usual onset | Before 35 years[1][2] |
| Causes | Unknown[1] |
| Risk factors | Child abuse, stress[2] |
| Diagnostic method | Based on the symptoms[2] |
| Differential diagnosis | Anxiety disorder, major depressive disorder, eating disorders, obsessive–compulsive personality disorder[2] |
| Treatment | Counseling, selective serotonin reuptake inhibitors, tricyclic antidepressants[4][5] |
| Frequency | 2.3%[6] |
Obsessive–compulsive disorder (OCD) is a mental disorder where people feel the need to check things repeatedly, perform certain routines repeatedly (called "rituals"), or have certain thoughts repeatedly (called "obsessions").[1] People are unable to control either the thoughts or the activities for more than a short period of time.[1] Common activities include hand washing, counting of things, and checking to see if a door is locked.[1] Some may have difficulty throwing things out.[1] These activities occur to such a degree that the person's daily life is negatively affected.[1] This often takes up more than an hour a day.[2] Most adults realize that the behaviors do not make sense.[1] The condition is associated with tics, anxiety disorder, and an increased risk of suicide.[2][3]
The cause is unknown.[1] There appear to be some genetic components with both identical twins more often affected than both non-identical twins.[2] Risk factors include a history of child abuse or other stress-inducing event.[2] Some cases have been documented to occur following infections.[2] The diagnosis is based on the symptoms and requires ruling out other drug related or medical causes.[2] Rating scales such as the Yale–Brown Obsessive Compulsive Scale (Y-BOCS) can be used to assess the severity.[7] Other disorders with similar symptoms include anxiety disorder, major depressive disorder, eating disorders, tic disorders, and obsessive–compulsive personality disorder.[2]
Treatment involves counseling, such as cognitive behavioral therapy (CBT), and sometimes antidepressants such as selective serotonin reuptake inhibitors (SSRIs) or clomipramine.[4][5] CBT for OCD involves increasing exposure to what causes the problems while not allowing the repetitive behavior to occur.[4] While clomipramine appears to work as well as SSRIs, it has greater side effects so is typically reserved as a second line treatment.[4]Atypical antipsychotics may be useful when used in addition to an SSRI in treatment-resistant cases but are also associated with an increased risk of side effects.[5][8] Without treatment, the condition often lasts decades.[2]
Obsessive–compulsive disorder affects about 2.3% of people at some point in their life.[6] Rates during a given year are about 1.2%, and it occurs worldwide.[2] It is unusual for symptoms to begin after the age of 35, and half of people develop problems before 20.[1][2] Males and females are affected about equally.[1] In English, the phrase obsessive–compulsive is often used in an informal manner unrelated to OCD to describe someone who is excessively meticulous, perfectionistic, absorbed, or otherwise fixated.[9]
.mw-parser-output .toclimit-2 .toclevel-1 ul,.mw-parser-output .toclimit-3 .toclevel-2 ul,.mw-parser-output .toclimit-4 .toclevel-3 ul,.mw-parser-output .toclimit-5 .toclevel-4 ul,.mw-parser-output .toclimit-6 .toclevel-5 ul,.mw-parser-output .toclimit-7 .toclevel-6 ul{display:none}
Contents
1 Signs and symptoms
1.1 Obsessions
1.2 Compulsions
1.3 Insight
1.4 Overvalued ideas
1.5 Cognitive performance
1.6 Children
2 Causes
2.1 Genetics
2.2 Autoimmune
3 Mechanisms
3.1 Neuroimaging
3.2 Cognitive models
3.3 Neurobiological
4 Diagnosis
4.1 Differential diagnosis
5 Management
5.1 Therapy
5.2 Medication
5.3 Procedures
5.4 Children
6 Epidemiology
6.1 Associated conditions
7 Prognosis
8 History
8.1 Notable cases
9 Society and culture
9.1 Art, entertainment and media
10 Research
11 Other animals
12 References
13 External links
Signs and symptoms
OCD can present with a wide variety of symptoms. Certain groups of symptoms usually occur together. These groups are sometimes viewed as dimensions or clusters that may reflect an underlying process. The standard assessment tool for OCD, the Yale–Brown Obsessive Compulsive Scale (Y-BOCS), has 13 predefined categories of symptoms. These symptoms fit into three to five groupings.[10] A meta analytic review of symptom structures found a four factor structure (grouping) to be most reliable. The observed groups included a "symmetry factor", a "forbidden thoughts factor", a "cleaning factor", and a "hoarding factor". The "symmetry factor" correlated highly with obsessions related to ordering, counting, and symmetry, as well as repeating compulsions. The "forbidden thoughts factor" correlated highly with intrusive and distressing thoughts of a violent, religious, or sexual nature. The "cleaning factor" correlated highly with obsessions about contamination and compulsions related to cleaning. The "hoarding factor" only involved hoarding-related obsessions and compulsions, and was identified as being distinct from other symptom groupings.[11]
While OCD has been considered a homogenous disorder from a neuropsychological perspective, many of the putative neuropsychological deficits may be due to comorbid disorders. Furthermore, some subtypes have been associated with improvement in performance on certain tasks such as pattern recognition (washing subtype) and spatial working memory (obsessive thought subtype). Subgroups have also been distinguished by neuroimaging findings and treatment response. Neuroimaging studies on this have been too few, and the subtypes examined have differed too much to draw any conclusions. On the other hand, subtype dependent treatment response has been studied, and the hoarding subtype has consistently responded least to treatment.[12]
Obsessions

People with OCD may face intrusive thoughts, such as thoughts about the Devil (shown is a painted interpretation of Hell)
Obsessions are thoughts that recur and persist, despite efforts to ignore or confront them.[13] People with OCD frequently perform tasks, or compulsions, to seek relief from obsession-related anxiety. Within and among individuals, the initial obsessions, or intrusive thoughts, vary in their clarity and vividness. A relatively vague obsession could involve a general sense of disarray or tension accompanied by a belief that life cannot proceed as normal while the imbalance remains. A more intense obsession could be a preoccupation with the thought or image of someone close to them dying[14][15] or intrusions related to "relationship rightness".[16] Other obsessions concern the possibility that someone or something other than oneself—such as God, the Devil, or disease—will harm either the person with OCD or the people or things that the person cares about. Other individuals with OCD may experience the sensation of invisible protrusions emanating from their bodies, or have the feeling that inanimate objects are ensouled.[17]
Some people with OCD experience sexual obsessions that may involve intrusive thoughts or images of "kissing, touching, fondling, oral sex, anal sex, intercourse, incest, and rape" with "strangers, acquaintances, parents, children, family members, friends, coworkers, animals, and religious figures", and can include "heterosexual or homosexual content" with persons of any age.[18] As with other intrusive, unpleasant thoughts or images, some disquieting sexual thoughts at times are normal, but people with OCD may attach extraordinary significance to the thoughts. For example, obsessive fears about sexual orientation can appear to the person with OCD, and even to those around them, as a crisis of sexual identity.[19][20] Furthermore, the doubt that accompanies OCD leads to uncertainty regarding whether one might act on the troubling thoughts, resulting in self-criticism or self-loathing.[18]
Most people with OCD understand that their notions do not correspond with reality; however, they feel that they must act as though their notions are correct. For example, an individual who engages in compulsive hoarding might be inclined to treat inorganic matter as if it had the sentience or rights of living organisms, while accepting that such behavior is irrational on a more intellectual level. There is a debate as to whether or not hoarding should be considered with other OCD symptoms.[21]
OCD sometimes manifests without overt compulsions, referred to as Primarily Obsessional OCD. OCD without overt compulsions could, by one estimate, characterize as many as 50 percent to 60 percent of OCD cases.[22]
Compulsions

Skin-picking disorder
Some people with OCD perform compulsive rituals because they inexplicably feel they have to, while others act compulsively so as to mitigate the anxiety that stems from particular obsessive thoughts. The person might feel that these actions somehow either will prevent a dreaded event from occurring or will push the event from their thoughts. In any case, the individual's reasoning is so idiosyncratic or distorted that it results in significant distress for the individual with OCD or for those around them. Excessive skin picking, hair-pulling, nail biting, and other body-focused repetitive behavior disorders are all on the obsessive–compulsive spectrum.[2] Some individuals with OCD are aware that their behaviors are not rational, but feel compelled to follow through with them to fend off feelings of panic or dread.[2][23]
Some common compulsions include hand washing, cleaning, checking things (e.g., locks on doors), repeating actions (e.g., turning on and off switches), ordering items in a certain way, and requesting reassurance.[24] Compulsions are different from tics (such as touching, tapping, rubbing, or blinking)[25] and stereotyped movements (such as head banging, body rocking, or self-biting), which usually aren't as complex and aren't precipitated by obsessions.[2] It can sometimes be difficult to tell the difference between compulsions and complex tics.[2] About 10% to 40% of individuals with OCD also have a lifetime tic disorder.[26]
People rely on compulsions as an escape from their obsessive thoughts; however, they are aware that the relief is only temporary, that the intrusive thoughts will soon return. Some people use compulsions to avoid situations that may trigger their obsessions. Although some people do certain things over and over again, they do not necessarily perform these actions compulsively. For example, bedtime routines, learning a new skill, and religious practices are not compulsions. Whether or not behaviors are compulsions or mere habit depends on the context in which the behaviors are performed. For example, arranging and ordering DVDs for eight hours a day would be expected of one who works in a video store, but would seem abnormal in other situations. In other words, habits tend to bring efficiency to one's life, while compulsions tend to disrupt it.[27]
In addition to the anxiety and fear that typically accompanies OCD, sufferers may spend hours performing such compulsions every day. In such situations, it can be hard for the person to fulfil their work, family, or social roles. In some cases, these behaviors can also cause adverse physical symptoms. For example, people who obsessively wash their hands with antibacterial soap and hot water can make their skin red and raw with dermatitis.[28]
People with OCD can use rationalizations to explain their behavior; however, these rationalizations do not apply to the overall behavior but to each instance individually. For example, a person compulsively checking the front door may argue that the time taken and stress caused by one more check of the front door is much less than the time and stress associated with being robbed, and thus checking is the better option. In practice, after that check, the person is still not sure and deems it is still better to perform one more check, and this reasoning can continue as long as necessary.
Insight
The DSM-V contains three specifiers for the level of insight in OCD. Good or fair insight is characterized by the acknowledgment that obsessive-compulsive beliefs are or may not be true. Poor insight is characterized by the belief that obsessive-complsive beliefs are probably true. Absence of insight make obsessive-compulsive beliefs delusional thoughts, and occurs in about 4% of people with OCD.[29]
Overvalued ideas
Some people with OCD exhibit what is known as overvalued ideas. In such cases, the person with OCD will truly be uncertain whether the fears that cause them to perform their compulsions are irrational or not. After some discussion, it is possible to convince the individual that their fears may be unfounded. It may be more difficult to do ERP therapy on such people because they may be unwilling to cooperate, at least initially. There are severe cases in which the person has an unshakeable belief in the context of OCD that is difficult to differentiate from psychotic disorders.[30]
Cognitive performance
A 2013 meta-analysis reported that people with OCD to have mild but wide-ranging cognitive deficits; significantly regarding spatial memory, to a lesser extent with verbal memory, fluency, executive function, and processing speed, while auditory attention was not significantly affected.[31] People with OCD show impairment in formulating an organizational strategy for coding information, set-shifting, and motor and cognitive inhibition.[32]
Specific subtypes of symptom dimensions in OCD have been associated with specific cognitive deficits.[33] For example, the results of one meta-analysis comparing washing and checking symptoms reported that washers outperformed checkers on eight out of ten cognitive tests.[34] The symptom dimension of contamination and cleaning may be associated with higher scores on tests of inhibition and verbal memory.[35]
Children
Approximately 1–2% of children are affected by OCD.[36] Obsessive–compulsive disorder symptoms tend to develop more frequently in children that are 10–14 years of age, with males displaying symptoms at an earlier age and a more severe level than the females.[37] In children, symptoms can be grouped into at least 4 types.[10]
Causes
The cause is unknown.[1] Both environmental and genetic factors are believed to play a role. Risk factors include a history of child abuse or other stress-inducing event.[2]
Genetics
There appear to be some genetic components with identical twins more often affected than non-identical twins.[2] Further, individuals with OCD are more likely to have first-degree family members exhibiting the same disorders than do matched controls. In cases where OCD develops during childhood, there is a much stronger familial link in the disorder than cases in which OCD develops later in adulthood. In general, genetic factors account for 45–65% of the variability in OCD symptoms in children diagnosed with the disorder.[38] A 2007 study found evidence supporting the possibility of a heritable risk for OCD.[39]
A mutation has been found in the human serotonin transporter gene, hSERT, in unrelated families with OCD.[40]
A systematic review found that while neither allele was associated with OCD overall, in caucasians the L allele was associated with OCD.[41] Another meta analysis observed an increased risk in those with the homozygous S allele, but found the LS genotype to be inversely associated with OCD.[42]
A genome wide association study found OCD to be linked with SNPs near BTBD3 and two SNPs in DLGAP1 in a trio-based analysis, but no SNP reached significance when analyzed with case-control data.[43]
One meta analysis found a small but significant association between a polymorphism in SLC1A1 and OCD.[44]
The relationship between OCD and COMT has been inconsistent, with one meta analysis reporting a significant association, albeit only in men,[45] and another meta analysis reporting no association.[46]
It has been postulated by evolutionary psychologists that moderate versions of compulsive behavior may have had evolutionary advantages. Examples would be moderate constant checking of hygiene, the hearth or the environment for enemies. Similarly, hoarding may have had evolutionary advantages. In this view OCD may be the extreme statistical "tail" of such behaviors, possibly due to a high amount of predisposing genes.[47]
Autoimmune
A controversial hypothesis[48] is that some cases of rapid onset of OCD in children and adolescents may be caused by a syndrome connected to Group A streptococcal infections, known as pediatric autoimmune neuropsychiatric disorders associated with streptococcal infections (PANDAS).[48][49]
A review of studies examining anti-basal ganglia antibodies in OCD found an increased risk of having anti-basal ganglia antibodies in those with OCD versus the general population.[50]
Mechanisms
Neuroimaging

Some parts of the brain showing abnormal activity in OCD.
Functional neuroimaging during symptom provocation has observed abnormal activity in the orbitofrontal cortex, left dorsolateral prefrontal cortex, right premotor cortex, left superior temporal gyrus, globus pallidus externus, hippocampus and right uncus. Weaker foci of abnormal activity were found in the left caudate, posterior cingulate cortex and superior parietal lobule.[51] However, an older meta analysis of functional neuroimaging in OCD reported the only consistent functional neuroimaging findings have been increased activity in the orbital gyrus and head of the caudate nucleus, while ACC activation abnormalities were too inconsistent.[52] A meta analysis comparing affective and non affective tasks observed differences with controls in regions implicated in salience, habit, goal-directed behavior, self-referential thinking and cognitive control. For non affective tasks, hyperactivity was observed in the insula, ACC, and head of the caudate/putamen, while hypoactivity was observed in the medial prefrontal cortex(mPFC) and posterior caudate. Affective tasks were observed to relate to increased activation in the precuneus and posterior cingulate cortex(PCC), while decreased activation was found in the pallidum, ventral anterior thalamus and postetior caudate.[53] The involvement of the cortico-striato-thalamo-cortical loop in OCD as well as the high rates of comorbidity between OCD and ADHD have led some to draw a link in their mechanism. Observed similarities include dysfunction of the anterior cingulate cortex, and prefrontal cortex, as well as shared deficits in executive functions.[54] The involvement of the orbitofrontal cortex and dorsolateral prefrontal cortex in OCD is shared with Bipolar Disorder and may explain their high degree of comorbidity.[55] Decreased volumes of the dorsolateral prefrontal cortex related to executive function has also been observed in OCD.[56]
People with OCD evince increased grey matter volumes in bilateral lenticular nuclei, extending to the caudate nuclei, with decreased grey matter volumes in bilateral dorsal medial frontal/anterior cingulate gyri.[57][58] These findings contrast with those in people with other anxiety disorders, who evince decreased (rather than increased) grey matter volumes in bilateral lenticular / caudate nuclei, as well as decreased grey matter volumes in bilateral dorsal medial frontal/anterior cingulate gyri.[58] Increased white matter volume and decreased fractional anisotropy in anterior midline tracts has been observed in OCD, possibly indicating increased fiber crossings.[59]
Cognitive models
Generally two categories of models for OCD have been postulated, the first involving deficits in executive function, and the second involving deficits in modulatory control. The first category of executive dysfunction is based on the observed structural and functional abnormalities in the dlPFC, striatum, and thalamus. The second category involving dysfunctional modulatory control primarily relies on observed functional and structural differences in the ACC, mPFC and OFC.[60][61]
One proposed model suggests that dysfunction in the OFC leads to improper valuation of behaviors and decreased behavioral control, while the observed alterations in amygdala activations leads to exaggerated fears and representations of negative stimuli.[62]
Due to the heterogeneity of OCD symptoms, studies differentiating between symptoms have been performed. Symptom specific neuroimaging abnormalities include the hyperactivity of caudate and ACC in checking rituals, while finding increased activity of cortical and cerebellar regions in contamination related symptoms. Neuroimaging differentiating between content of intrusive thoughts have found differences between aggressive as opposed to taboo thoughts, finding increased connectivity of the amygdala, ventral striatum, and ventromedial prefrontal cortex in aggressive symptoms, while observing increased connectivity between the ventral striatum and insula in sexual/religious intrusive thoughts.[63]
Another model proposes that affective dysregulation links excessive reliance on habit based action selection[64] with compulsions. This is supported by the observation that those with OCD demonstrate decreased activation of the ventral striatum when anticipating monetary reward, as well as increase functional connectivity between the VS and the OFC. Furthermore, those with OCD demonstrate reduced performance in pavlovian fear extinction tasks, hyper responsiveness in the amygdala to fearful stimuli, and hypo-responsiveness in the amygdala when exposed to positively valanced stimuli. Stimulation of the nucleus accumbens has also been observed to effectively alleviate both obsessions and compulsions, supporting the role of affective dysregulation in generating both.[62]
Neurobiological
From the observation of the efficacy of antidepressants in OCD, a serotonin hypothesis of OCD has been formulated. Studies of peripheral markers of serotonin, as well as challenges with proserotonergic compounds have yielded inconsistent results, including evidence pointing towards basal hyperactivity of serotonergic systems.[65] Serotonin receptor and transporter binding studies have yielded conflicting results, including higher and lower serotonin receptor 5-HT2A and serotonin transporter binding potentials that were normalized by treatment with SSRIs. Despite inconsistencies in the types of abnormalities found, evidence points towards dysfunction of serotonergic systems in OCD.[66]Orbitofrontal cortex overactivity is attenuated in people who have successfully responded to SSRI medication, a result believed to be caused by increased stimulation of serotonin receptors 5-HT2A and 5-HT2C.[67] A complex relationship between dopamine and OCD has been observed. Although antipsychotics, which act by antagonizing dopamine receptors may improve some cases of OCD, they frequently exacerbate others. Antipsychotics, in the low doses used to treat OCD, may actually increased the release of dopamine in the prefrontal cortex, through inhibiting autoreceptors. Further complicating things is the efficacy of amphetamines, decreased dopamine transporter activity observed in OCD,[68] and low levels of D2 binding in the striatum.[69] Furthermore, increased dopamine release in the nucleus accumbens after deep brain stimulation correlates with improvement in symptoms, pointing to reduced dopamine release in the striatum playing a role in generating symptoms.[70]
Abnormalities in glutaminergic neurotransmission have implicated in OCD. Findings such as increased cerebrospinal glutamate, less consistent abnormalities observed in neuroimaging studies, and the efficacy of some glutaminergic drugs such as riluzole have implicated glutamate in OCD.[69] OCD has been associated with reduced N-Acetylaspartic acid in the mPFC, which is thought to reflect neuron density or functionality, although the exact interpretation has not been established.[71]
Diagnosis
Formal diagnosis may be performed by a psychologist, psychiatrist, clinical social worker, or other licensed mental health professional. To be diagnosed with OCD, a person must have obsessions, compulsions, or both, according to the Diagnostic and Statistical Manual of Mental Disorders (DSM). The Quick Reference to the 2000 edition of the DSM states that several features characterize clinically significant obsessions and compulsions. Such obsessions, the DSM says, are recurrent and persistent thoughts, impulses or images that are experienced as intrusive and that cause marked anxiety or distress. These thoughts, impulses or images are of a degree or type that lies outside the normal range of worries about conventional problems.[72] A person may attempt to ignore or suppress such obsessions, or to neutralize them with some other thought or action, and will tend to recognize the obsessions as idiosyncratic or irrational.
Compulsions become clinically significant when a person feels driven to perform them in response to an obsession, or according to rules that must be applied rigidly, and when the person consequently feels or causes significant distress. Therefore, while many people who do not suffer from OCD may perform actions often associated with OCD (such as ordering items in a pantry by height), the distinction with clinically significant OCD lies in the fact that the person who suffers from OCD must perform these actions, otherwise they will experience significant psychological distress. These behaviors or mental acts are aimed at preventing or reducing distress or preventing some dreaded event or situation; however, these activities are not logically or practically connected to the issue, or they are excessive. In addition, at some point during the course of the disorder, the individual must realize that their obsessions or compulsions are unreasonable or excessive.
Moreover, the obsessions or compulsions must be time-consuming (taking up more than one hour per day) or cause impairment in social, occupational or scholastic functioning.[72] It is helpful to quantify the severity of symptoms and impairment before and during treatment for OCD. In addition to the peron's estimate of the time spent each day harboring obsessive-compulsive thoughts or behaviors, concrete tools can be used to gauge the people’s condition. This may be done with rating scales, such as the Yale–Brown Obsessive Compulsive Scale (Y-BOCS). With measurements like these, psychiatric consultation can be more appropriately determined because it has been standardized.[7]
OCD is sometimes placed in a group of disorders called the obsessive–compulsive spectrum.[73]
Differential diagnosis
OCD is often confused with the separate condition obsessive–compulsive personality disorder (OCPD). OCD is egodystonic, meaning that the disorder is incompatible with the sufferer's self-concept.[74][75] Because ego dystonic disorders go against a person's self-concept, they tend to cause much distress. OCPD, on the other hand, is egosyntonic—marked by the person's acceptance that the characteristics and behaviours displayed as a result are compatible with their self-image, or are otherwise appropriate, correct or reasonable.
As a result, people with OCD are often aware that their behavior is not rational, are unhappy about their obsessions but nevertheless feel compelled by them.[76] By contrast people with OCPD are not aware of anything abnormal; they will readily explain why their actions are rational, it is usually impossible to convince them otherwise, and they tend to derive pleasure from their obsessions or compulsions.[76]
Management
A form of psychotherapy called "cognitive behavioral therapy" (CBT) and psychotropic medications are first-line treatments for OCD.[1][77] Other forms of psychotherapy, such as psychodynamic and psychoanalysis may help in managing some aspects of the disorder, but in 2007 the American Psychiatric Association (APA) noted a lack of controlled studies showing their effectiveness "in dealing with the core symptoms of OCD".[78] The fact that many individuals do not seek treatment may be due in part to stigma associated with OCD.[citation needed]
Therapy

One exposure and ritual prevention activity would be to check the lock only once, and then leave
The specific technique used in CBT is called exposure and response prevention (ERP) which involves teaching the person to deliberately come into contact with the situations that trigger the obsessive thoughts and fears ("exposure"), without carrying out the usual compulsive acts associated with the obsession ("response prevention"), thus gradually learning to tolerate the discomfort and anxiety associated with not performing the ritualistic behavior. At first, for example, someone might touch something only very mildly "contaminated" (such as a tissue that has been touched by another tissue that has been touched by the end of a toothpick that has touched a book that came from a "contaminated" location, such as a school.) That is the "exposure". The "ritual prevention" is not washing. Another example might be leaving the house and checking the lock only once (exposure) without going back and checking again (ritual prevention). The person fairly quickly habituates to the anxiety-producing situation and discovers that their anxiety level drops considerably; they can then progress to touching something more "contaminated" or not checking the lock at all—again, without performing the ritual behavior of washing or checking.[79]
ERP has a strong evidence base, and it is considered the most effective treatment for OCD.[79] However, this claim was doubted by some researchers in 2000 who criticized the quality of many studies.[80]
It has generally been accepted that psychotherapy, in combination with psychiatric medication, is more effective than either option alone.
Medication

A blister pack of clomipramine under the brand name Anafranil
The medications most frequently used are the selective serotonin reuptake inhibitors (SSRIs).[4]Clomipramine, a medication belonging to the class of tricyclic antidepressants, appears to work as well as SSRIs but has a higher rate of side effects.[4]
SSRIs are a second line treatment of adult obsessive compulsive disorder (OCD) with mild functional impairment and as first line treatment for those with moderate or severe impairment. In children, SSRIs can be considered as a second line therapy in those with moderate-to-severe impairment, with close monitoring for psychiatric adverse effects.[77] SSRIs are efficacious in the treatment of OCD; people treated with SSRIs are about twice as likely to respond to treatment as those treated with placebo.[81][82] Efficacy has been demonstrated both in short-term (6–24 weeks) treatment trials and in discontinuation trials with durations of 28–52 weeks.[83][84][85]
In 2006, the National Institute of Clinical and Health Excellence (NICE) guidelines recommended antipsychotics for OCD that does not improve with SSRI treatment.[5] For OCD there is tentative evidence for risperidone and insufficient evidence for olanzapine. Quetiapine is no better than placebo with regard to primary outcomes, but small effects were found in terms of YBOCS score. The efficacy of quetiapine and olanzapine are limited by the insufficient number of studies.[86] A 2014 review article found two studies that indicated that aripiprazole was "effective in the short-term" and found that "[t]here was a small effect-size for risperidone or anti-psychotics in general in the short-term"; however, the study authors found "no evidence for the effectiveness of quetiapine or olanzapine in comparison to placebo."[5] While quetiapine may be useful when used in addition to an SSRI in treatment-resistant OCD, these drugs are often poorly tolerated, and have metabolic side effects that limit their use. None of the atypical antipsychotics appear to be useful when used alone.[8] Another review reported that no evidence supports the use of first generation antipsychotics in OCD.[87]
A guideline by the APA suggested that dextroamphetamine may be considered by itself after more well supported treatments have been tried.[88]
Procedures
Electroconvulsive therapy (ECT) has been found to have effectiveness in some severe and refractory cases.[89]
Surgery may be used as a last resort in people who do not improve with other treatments. In this procedure, a surgical lesion is made in an area of the brain (the cingulate cortex). In one study, 30% of participants benefitted significantly from this procedure.[90]Deep-brain stimulation and vagus nerve stimulation are possible surgical options that do not require destruction of brain tissue. In the United States, the Food and Drug Administration approved deep-brain stimulation for the treatment of OCD under a humanitarian device exemption requiring that the procedure be performed only in a hospital with specialist qualifications to do so.[91]
In the United States, psychosurgery for OCD is a treatment of last resort and will not be performed until the person has failed several attempts at medication (at the full dosage) with augmentation, and many months of intensive cognitive–behavioral therapy with exposure and ritual/response prevention.[92] Likewise, in the United Kingdom, psychosurgery cannot be performed unless a course of treatment from a suitably qualified cognitive–behavioral therapist has been carried out.
Children
Therapeutic treatment may be effective in reducing ritual behaviors of OCD for children and adolescents.[93] Similar to the treatment of adults with OCD, CBT stands as an effective and validated first line of treatment of OCD in children.[94] Family involvement, in the form of behavioral observations and reports, is a key component to the success of such treatments.[95] Parental interventions also provide positive reinforcement for a child who exhibits appropriate behaviors as alternatives to compulsive responses. In a recent meta-analysis of evidenced-based treatment of OCD in children, family-focused individual CBT was labeled as "probably efficacious", establishing it as one of the leading psychosocial treatments for youth with OCD.[94] After one or two years of therapy, in which a child learns the nature of his or her obsession and acquires strategies for coping, that child may acquire a larger circle of friends, exhibit less shyness, and become less self-critical.[96]
Although the causes of OCD in younger age groups range from brain abnormalities to psychological preoccupations, life stress such as bullying and traumatic familial deaths may also contribute to childhood cases of OCD, and acknowledging these stressors can play a role in treating the disorder.[97]
Epidemiology
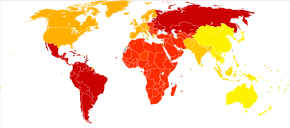
Age-standardized disability-adjusted life year estimated rates for obsessive-compulsive disorder per 100,000 inhabitants in 2004..mw-parser-output .refbegin{font-size:90%;margin-bottom:0.5em}.mw-parser-output .refbegin-hanging-indents>ul{list-style-type:none;margin-left:0}.mw-parser-output .refbegin-hanging-indents>ul>li,.mw-parser-output .refbegin-hanging-indents>dl>dd{margin-left:0;padding-left:3.2em;text-indent:-3.2em;list-style:none}.mw-parser-output .refbegin-100{font-size:100%}
no data
<45
45–52.5
52.5–60
60–67.5
67.5–75
75–82.5
82.5–90
90–97.5
97.5–105
105–112.5
112.5–120
>120
Obsessive–compulsive disorder affects about 2.3% of people at some point in their life.[6] Rates during a given year are about 1.2% and it occurs worldwide.[2] It is unusual for symptoms to begin after the age of thirty five and half of people develop problems before twenty.[1][2] Males and females are affected about equally.[1]
Associated conditions
People with OCD may be diagnosed with other conditions, as well as or instead of OCD, such as the aforementioned obsessive–compulsive personality disorder, major depressive disorder, bipolar disorder,[98]generalized anxiety disorder, anorexia nervosa, social anxiety disorder, bulimia nervosa, Tourette syndrome, autism spectrum disorder, attention deficit hyperactivity disorder, dermatillomania (compulsive skin picking), body dysmorphic disorder and trichotillomania (hair pulling). More than 50 percent of people experience suicidal tendencies, and 15 percent have attempted suicide.[7] Depression, anxiety and prior suicide attempts increase the risk of future suicide attempts.[99]
Individuals with OCD have also been found to be affected by delayed sleep phase syndrome at a substantially higher rate than the general public.[100] Moreover, severe OCD symptoms are consistently associated with greater sleep disturbance. Reduced total sleep time and sleep efficiency have been observed in people with OCD, with delayed sleep onset and offset and an increased prevalence of delayed sleep phase disorder.[101]
Behaviorally, there is some research demonstrating a link between drug addiction and the disorder as well. For example, there is a higher risk of drug addiction among those with any anxiety disorder (possibly as a way of coping with the heightened levels of anxiety), but drug addiction among people with OCD may serve as a type of compulsive behavior and not just as a coping mechanism. Depression is also extremely prevalent among people with OCD. One explanation for the high depression rate among OCD populations was posited by Mineka, Watson and Clark (1998), who explained that people with OCD (or any other anxiety disorder) may feel depressed because of an "out of control" type of feeling.[102]
Someone exhibiting OCD signs does not necessarily have OCD. Behaviors that present as (or seem to be) obsessive or compulsive can also be found in a number of other conditions as well, including obsessive–compulsive personality disorder (OCPD), autism spectrum disorder, disorders where perseveration is a possible feature (ADHD, PTSD, bodily disorders or habit problems)[103] or sub-clinically.
Some with OCD present with features typically associated with Tourette's syndrome, such as compulsions that may appear to resemble motor tics; this has been termed "tic-related OCD" or "Tourettic OCD".[104][105]
A myth propagated by Sigmund Freud regarding above-average intelligence in OCD was recently refuted.[106]
OCD frequently co-occurs with both bipolar disorder and major depressive disorder. Between 60–80% of those with OCD experience a major depressive episode in their lifetime. Comorbidity rates have been reported at between 19–90% due to methodological differences. Between 9–35% of those with bipolar disorder also have OCD, compared to the 1–2% in the general population. Around 50% of those with OCD experience cyclothymic traits or hypomanic episodes. OCD is also associated with anxiety disorders. Lifetime comorbidity for OCD has been reported at 22% for specific phobia, 18% for social anxiety disorder, 12% for panic disorder, and 30% for generalized anxiety disorder. The comorbidity rate for OCD and ADHD has been reported as high as 51%.[107]
Prognosis
Quality of life is reduced across all domains in OCD. While psychological or pharmacological treatment can lead to a reduction of OCD symptoms and an increase in QoL, symptoms may persist at moderate levels even following adequate treatment courses, and completely symptom-free periods are uncommon.[108][109] In pediatric OCD, around 40% still have the disorder in adulthood, and around 40% qualify for remission.[110]
History
In the seventh century AD, John Climacus records an instance of a young monk plagued by constant and overwhelming "temptations to blasphemy" consulting an older monk,[111]:212 who told him, "My son, I take upon myself all the sins which these temptations have led you, or may lead you, to commit. All I require of you is that for the future you pay no attention to them whatosever."[111]:212The Cloud of Unknowing, a Christian mystical text from the late fourteenth century, recommends dealing with recurring obsessions by first attempting to ignore them,[111]:213 and, if that fails, "cower under them like a poor wretch and a coward overcome in battle, and reckon it to be a waste of your time for you to strive any longer against them",[111]:213 a technique now known as "emotional flooding".[111]:213
From the 14th to the 16th century in Europe, it was believed that people who experienced blasphemous, sexual or other obsessive thoughts were possessed by the Devil.[74][111]:213 Based on this reasoning, treatment involved banishing the "evil" from the "possessed" person through exorcism.[112][113] The vast majority of people who thought they were possessed by the Devil did not suffer from hallucinations or other "spectacular symptoms",[111]:213 but "complained of anxiety, religious fears, and evil thoughts."[111]:213 In 1584, a woman from Kent, England named Mrs. Davie, described by a justice of the peace as "a good wife",[111]:213 was nearly burned at the stake after she confessed that she experienced constant, unwanted urges to murder her family.[111]:213
The English term obsessive-compulsive comes from the translated term used to describe the first conceptions of OCD by Carl Westphal, "zwangsvorstellung". Westphal's description went on to influence Pierre Janet who further documented features of OCD.[29] In the early 1910s, Sigmund Freud attributed obsessive–compulsive behavior to unconscious conflicts that manifest as symptoms.[112] Freud describes the clinical history of a typical case of "touching phobia" as starting in early childhood, when the person has a strong desire to touch an item. In response, the person develops an "external prohibition" against this type of touching. However, this "prohibition does not succeed in abolishing" the desire to touch; all it can do is repress the desire and "force it into the unconscious".[114] Freudian psychoanalysis remained the dominant treatment for OCD until the mid-1980s,[111]:210–211 even though medicinal and therapeutical treatments were known and available,[111]:210 because it was widely thought that these treatments would be detrimental to the effectiveness of the psychotherapy.[111]:210 In the mid-1980s, psychiatry made a sudden "about-face" on the subject[111]:210 and began treating OCD primarily through medicine and practical therapy rather than psychoanalysis.[111]:210
Notable cases
John Bunyan (1628–1688), the author of The Pilgrim's Progress, displayed symptoms of OCD (which had not yet been named).[111]:53–54 During the most severe period of his condition, he would mutter the same phrase over and over again to himself while rocking back and forth.[111]:53–54 He later described his obsessions in his autobiography Grace Abounding to the Chief of Sinners,[111]:53–54 stating, "These things may seem ridiculous to others, even as ridiculous as they were in themselves, but to me they were the most tormenting cogitations."[111]:54 He wrote two pamphlets advising those suffering from similar anxieties.[111]:217–218 In one of them, he warns against indulging in compulsions:[111]:217–218 "Have care of putting off your trouble of spirit in the wrong way: by promising to reform yourself and lead a new life, by your performances or duties".[111]:218
British poet, essayist and lexicographer Samuel Johnson (1709–1784) also suffered from OCD.[111]:54–55 He had elaborate rituals for crossing the thresholds of doorways, and repeatedly walked up and down staircases counting the steps.[115][111]:55 He would touch every post on the street as he walked past,[111]:55 only step in the middles of paving stones,[111]:55 and repeatedly perform tasks as though they had not been done properly the first time.[111]:55 The American aviator and filmmaker Howard Hughes is known to have had OCD.[116] Friends of Hughes have also mentioned his obsession with minor flaws in clothing.[117] This was conveyed in The Aviator (2004), a film biography of Hughes.[118]
Society and culture

This ribbon represents Trichotillomania and other body focused repetitive behaviors. Concept for the ribbon was started by Jenne Schrader. Colors were voted on by the Trichotillomania Facebook community, and made official by Trichotillomania Learning Center in August 2013.
Art, entertainment and media
Movies and television shows often portray idealized representations of disorders such as OCD. These depictions may lead to increased public awareness, understanding and sympathy for such disorders.[119]
- In the film As Good as It Gets (1997), actor Jack Nicholson portrays a man "with Obsessive Compulsive Disorder (OCD)".[120] "Throughout the film, [he] engages in ritualistic behaviors (i.e., compulsions) that disrupt his interpersonal and professional life", a "cinematic representation of psychopathology [that] accurately depicts the functional interference and distress associated with OCD".[120]
- The film Matchstick Men (2003), directed by Ridley Scott, portrays a con-man named Roy (Nicolas Cage) who has obsessive-compulsive disorder. The film "opens with Roy, at home, suffering with his numerous obsessive compulsive symptoms, which take the form of a need for order and cleanliness and a compulsion to open and close doors three times, whilst counting aloud, before he can walk through them".[121]
- In the USA Network American comedy-drama detective mystery television series Monk (2002–2009), the titular Adrian Monk fears both human contact and dirt.[122][123]
Research
The naturally occurring sugar inositol has been suggested as a treatment for OCD.[124]
Nutrition deficiencies may also contribute to OCD and other mental disorders. Vitamin and mineral supplements may aid in such disorders and provide nutrients necessary for proper mental functioning.[125]
μ-Opioids, such as hydrocodone and tramadol, may improve OCD symptoms.[126] Administration of opiate treatment may be contraindicated in individuals concurrently taking CYP2D6 inhibitors such as fluoxetine and paroxetine.[127]
Much current research is devoted to the therapeutic potential of the agents that affect the release of the neurotransmitter glutamate or the binding to its receptors. These include riluzole,[128]memantine, gabapentin, N-acetylcysteine, topiramate and lamotrigine.[citation needed]
Other animals
References
^ abcdefghijklmnop The National Institute of Mental Health (NIMH) (January 2016). "What is Obsessive-Compulsive Disorder (OCD)?". U.S. National Institutes of Health (NIH). Archived from the original on 23 July 2016. Retrieved 24 July 2016..mw-parser-output cite.citation{font-style:inherit}.mw-parser-output q{quotes:"""""""'""'"}.mw-parser-output code.cs1-code{color:inherit;background:inherit;border:inherit;padding:inherit}.mw-parser-output .cs1-lock-free a{background:url("//upload.wikimedia.org/wikipedia/commons/thumb/6/65/Lock-green.svg/9px-Lock-green.svg.png")no-repeat;background-position:right .1em center}.mw-parser-output .cs1-lock-limited a,.mw-parser-output .cs1-lock-registration a{background:url("//upload.wikimedia.org/wikipedia/commons/thumb/d/d6/Lock-gray-alt-2.svg/9px-Lock-gray-alt-2.svg.png")no-repeat;background-position:right .1em center}.mw-parser-output .cs1-lock-subscription a{background:url("//upload.wikimedia.org/wikipedia/commons/thumb/a/aa/Lock-red-alt-2.svg/9px-Lock-red-alt-2.svg.png")no-repeat;background-position:right .1em center}.mw-parser-output .cs1-subscription,.mw-parser-output .cs1-registration{color:#555}.mw-parser-output .cs1-subscription span,.mw-parser-output .cs1-registration span{border-bottom:1px dotted;cursor:help}.mw-parser-output .cs1-hidden-error{display:none;font-size:100%}.mw-parser-output .cs1-visible-error{font-size:100%}.mw-parser-output .cs1-subscription,.mw-parser-output .cs1-registration,.mw-parser-output .cs1-format{font-size:95%}.mw-parser-output .cs1-kern-left,.mw-parser-output .cs1-kern-wl-left{padding-left:0.2em}.mw-parser-output .cs1-kern-right,.mw-parser-output .cs1-kern-wl-right{padding-right:0.2em}
^ abcdefghijklmnopqrstuvw Diagnostic and statistical manual of mental disorders : DSM-5 (5 ed.). Washington: American Psychiatric Publishing. 2013. pp. 237–242. ISBN 978-0-89042-555-8.
^ ab Angelakis, I; Gooding, P; Tarrier, N; Panagioti, M (25 March 2015). "Suicidality in obsessive compulsive disorder (OCD): A systematic review and meta-analysis". Clinical Psychology Review. Oxford, England: Pergamon Press. 39: 1–15. doi:10.1016/j.cpr.2015.03.002. PMID 25875222.
^ abcdef Grant JE (14 August 2014). "Clinical practice: Obsessive-compulsive disorder". The New England Journal of Medicine. 371 (7): 646–53. doi:10.1056/NEJMcp1402176. PMID 25119610.
^ abcde Veale, D; Miles, S; Smallcombe, N; Ghezai, H; Goldacre, B; Hodsoll, J (29 November 2014). "Atypical antipsychotic augmentation in SSRI treatment refractory obsessive-compulsive disorder: a systematic review and meta-analysis". BMC Psychiatry. 14: 317. doi:10.1186/s12888-014-0317-5. PMC 4262998. PMID 25432131.
^ abc Goodman, WK; Grice, DE; Lapidus, KA; Coffey, BJ (September 2014). "Obsessive-compulsive disorder". The Psychiatric Clinics of North America. 37 (3): 257–67. doi:10.1016/j.psc.2014.06.004. PMID 25150561.
^ abc Fenske JN, Schwenk TL (August 2009). "Obsessive compulsive disorder: diagnosis and management". American Family Physician. 80 (3): 239–45. PMID 19621834. Archived from the original on 12 May 2014.
^ ab Decloedt EH, Stein DJ (2010). "Current trends in drug treatment of obsessive-compulsive disorder". Neuropsychiatr Dis Treat. 6: 233–42. doi:10.2147/NDT.S3149. PMC 2877605. PMID 20520787.
^ Bynum, W.F.; Porter, Roy; Shepherd, Michael (1985). "Obsessional Disorders: A Conceptual History. Terminological and Classificatory Issues.". The anatomy of madness : essays in the history of psychiatry. London: Routledge. pp. 166–187. ISBN 978-0-415-32382-6.
^ ab Leckman, JF; Bloch, MH; King, RA (2009). "Symptom dimensions and subtypes of obsessive-compulsive disorder: a developmental perspective". Dialogues in Clinical Neuroscience. 11 (1): 21–33. PMC 3181902. PMID 19432385.
^ Bloch, MH; Landeros-Weisenberger, A; Rosario, MC; Pittenger, C; Leckman, JF (December 2008). "Meta-analysis of the symptom structure of obsessive-compulsive disorder". The American Journal of Psychiatry. 165 (12): 1532–42. doi:10.1176/appi.ajp.2008.08020320. PMC 3972003. PMID 18923068.
^ McKay, D; Abramowitz, JS; Calamari, JE; Kyrios, M; Radomsky, A; Sookman, D; Taylor, S; Wilhelm, S (July 2004). "A critical evaluation of obsessive-compulsive disorder subtypes: symptoms versus mechanisms". Clinical Psychology Review. 24 (3): 283–313. doi:10.1016/j.cpr.2004.04.003. PMID 15245833.
^ Markarian, Y; Larson, MJ; Aldea, MA; Baldwin, SA; Good, D; Berkeljon, A; Murphy, TK; Storch, EA; McKay, D (February 2010). "Multiple pathways to functional impairment in obsessive-compulsive disorder". Clinical Psychology Review. 30 (1): 78–88. doi:10.1016/j.cpr.2009.09.005. PMID 19853982.
^ Baer 2001, pp. 33, 78.
^ Baer 2001, p. xiv.
^ Doron, G; Szepsenwol, O; Karp, E; Gal, N (2013). "Obsessing About Intimate-Relationships: Testing the Double Relationship-Vulnerability Hypothesis". Journal of Behavior Therapy and Experimental Psychiatry. 44 (4): 433–440. doi:10.1016/j.jbtep.2013.05.003. PMID 23792752.
^ Mash, Eric J.; Wolfe, David A. (2005). Abnormal child psychology (3 ed.). Belmont, California: Thomson Wadsworth. p. 197. ISBN 978-1305105423.
^ ab Osgood-Hynes, Deborah. "Thinking Bad Thoughts" (PDF). Belmont, Massachusetts: MGH/McLean OCD Institute. Archived from the original (PDF) on November 15, 2011. Retrieved December 30, 2006.
^ Phillipson, Steven. "I Think It Moved". OCDOnline.com. New York City: Center for Cognitive-Behavioral Psychotherapy. Archived from the original on December 18, 2008. Retrieved May 14, 2009.
^ Johnson, Mark-Ameen. "I'm Gay and You're Not : Understanding Homosexuality Fears". brainphysics.com. Archived from the original on 5 May 2009. Retrieved 14 May 2009.
^ Murphy, DL; Timpano, KR; Wheaton, MG; Greenberg, BD; Miguel, EC (2010). "Obsessive-compulsive disorder and its related disorders: a reappraisal of obsessive-compulsive spectrum concepts". Dialogues in Clinical Neuroscience. 12 (2): 131–48. PMC 3181955. PMID 20623919.
^ Weisman, Myrna M. (May 1998). "The cross national epidemiology of obsessive–compulsive disorder". New Developments in Obsessive-Compulsive and Spectrum Disorders. 3 (1): 6–9.
^ Highlights of Changes from DSM-IV-TR to DSM-5 (PDF), American Psychiatric Association, 2013, p. 7, archived (PDF) from the original on 19 October 2013, retrieved 12 April 2016
^ Boyd MA (2007). Psychiatric Nursing. Issues in Mental Health Nursing. 15. Lippincott Williams & Wilkins. pp. 13–26. ISBN 978-0-397-55178-1. PMID 8119793.
^ Storch; et al. (2008). "Obsessive-compulsive disorder in youth with and without a chronic tic disorder". Depression and Anxiety. 25 (9): 761–767. doi:10.1002/da.20304. PMID 17345600.
^ Conelea; et al. (2014), "Tic-related obsessive-compulsive disorder (OCD): phenomenology and treatment outcome in the Pediatric OCD Treatment Study II", Journal of the American Academy of Child & Adolescent Psychiatry, 53 (12): 1308–16, doi:10.1016/j.jaac.2014.09.014, PMC 4254546, PMID 25457929
^ "Obsessive-Compulsive Disorder, (2005)". Retrieved 15 December 2009.
^ "Hygiene of the Skin: When Is Clean Too Clean? Subtopic: "Skin Barrier Properties and Effect of Hand Hygiene Practices", Paragraph 5". Archived from the original on 21 April 2009. Retrieved 26 March 2009.
^ ab Ruiz, P; Sadock, B; Sadock, V (2017). Kaplan and Sadock's Comprehensive Textbook of Psychiatry (10th ed.). 95218: LWW. ISBN 978-1-4511-0047-1.
^ O'Dwyer, Anne-Marie Carter, Obsessive–compulsive disorder and delusions revisited, The British Journal of Psychiatry (2000) 176: 281–284
^ Shin NY, Lee TY, Kim E, Kwon JS (19 July 2013). "Cognitive functioning in obsessive-compulsive disorder: a meta-analysis". Psychological Medicine. 44 (6): 1–10. doi:10.1017/S0033291713001803. PMID 23866289.
^ Çetinay Aydın P, Güleç Öyekçin D (2013). "Cognitive functions in patients with obsessive compulsive disorder". Turk Psikiyatri Dergisi (Turkish Journal of Psychiatry). 24 (4): 266–74. doi:10.5080/u7172. PMID 24310094.
^ Pauls, DL; Abramovitch, A; Rauch, SL; Geller, DA (June 2014). "Obsessive-compulsive disorder: an integrative genetic and neurobiological perspective". Nature Reviews. Neuroscience. 15 (6): 410–24. doi:10.1038/nrn3746. PMID 24840803.
^ Leopold, R; Backenstrass, M (March 2015). "Neuropsychological differences between obsessive-compulsive washers and checkers: a systematic review and meta-analysis". Journal of Anxiety Disorders. 30: 48–58. doi:10.1016/j.janxdis.2014.12.016. PMID 25601381.
^ Abramovitch, Amitai; Cooperman, Allison (April 2015). "The cognitive neuropsychology of obsessive-compulsive disorder: A critical review". Journal of Obsessive-Compulsive and Related Disorders. 5: 24–36. doi:10.1016/j.jocrd.2015.01.002.
^ Jones, Anna M.; Nadai, Alessandro S. De; Arnold, Elysse B.; McGuire, Joseph F.; Lewin, Adam B.; Murphy, Tanya K.; Storch, Eric A. (2013-02-01). "Psychometric Properties of the Obsessive Compulsive Inventory: Child Version in Children and Adolescents with Obsessive–Compulsive Disorder". Child Psychiatry & Human Development. 44 (1): 137–151. doi:10.1007/s10578-012-0315-0. ISSN 0009-398X. PMID 22711294.
^ Last, Cynthia G.; Strauss, Cyd C. (1989). "Obsessive—compulsive disorder in childhood". Journal of Anxiety Disorders. 3 (4): 295–302. doi:10.1016/0887-6185(89)90020-0.
^ Abramowitz JS, Taylor S, McKay D (2009). "Obsessive-compulsive disorder". Lancet. 374 (9688): 491–9. doi:10.1016/S0140-6736(09)60240-3. PMID 19665647.
^ Menzies L, Achard S, Chamberlain SR, Fineberg N, Chen CH, del Campo N, Sahakian BJ, Robbins TW, Bullmore E (2007). "Neurocognitive endophenotypes of obsessive-compulsive disorder". Brain. 130 (Pt 12): 3223–36. doi:10.1093/brain/awm205. PMID 17855376.CS1 maint: Uses authors parameter (link)
^ Ozaki N, Goldman D, Kaye WH, Plotnicov K, Greenberg BD, Lappalainen J, Rudnick G, Murphy DL (2003). "Serotonin transporter missense mutation associated with a complex neuropsychiatric phenotype". Mol. Psychiatry. 8 (11): 933–6. doi:10.1038/sj.mp.4001365. PMID 14593431.
^ Bloch, MH; Landeros-Weisenberger, A; Sen, S; Dombrowski, P; Kelmendi, B; Coric, V; Pittenger, C; Leckman, JF (5 September 2008). "Association of the serotonin transporter polymorphism and obsessive-compulsive disorder: systematic review". American Journal of Medical Genetics. Part B, Neuropsychiatric Genetics. 147B (6): 850–8. doi:10.1002/ajmg.b.30699. PMID 18186076.
^ Lin, PY (13 April 2007). "Meta-analysis of the association of serotonin transporter gene polymorphism with obsessive-compulsive disorder". Progress in Neuro-psychopharmacology & Biological Psychiatry. 31 (3): 683–9. doi:10.1016/j.pnpbp.2006.12.024. PMID 17291658.
^ Stewart, SE; Yu, D; Scharf, JM; Neale, BM; Fagerness, JA; Mathews, CA; Arnold, PD; Evans, PD; Gamazon, ER; Davis, LK; Osiecki, L; McGrath, L; Haddad, S; Crane, J; Hezel, D; Illman, C; Mayerfeld, C; Konkashbaev, A; Liu, C; Pluzhnikov, A; Tikhomirov, A; Edlund, CK; Rauch, SL; Moessner, R; Falkai, P; Maier, W; Ruhrmann, S; Grabe, HJ; Lennertz, L; et al. (July 2013). "Genome-wide association study of obsessive-compulsive disorder". Molecular Psychiatry. 18 (7): 788–98. doi:10.1038/mp.2012.85. PMC 4218751. PMID 22889921.
^ Stewart, SE; Mayerfeld, C; Arnold, PD; Crane, JR; O'Dushlaine, C; Fagerness, JA; Yu, D; Scharf, JM; Chan, E; Kassam, F; Moya, PR; Wendland, JR; Delorme, R; Richter, MA; Kennedy, JL; Veenstra-VanderWeele, J; Samuels, J; Greenberg, BD; McCracken, JT; Knowles, JA; Fyer, AJ; Rauch, SL; Riddle, MA; Grados, MA; Bienvenu, OJ; Cullen, B; Wang, Y; Shugart, YY; Piacentini, J; Rasmussen, S; Nestadt, G; Murphy, DL; Jenike, MA; Cook, EH; Pauls, DL; Hanna, GL; Mathews, CA (June 2013). "Meta-analysis of association between obsessive-compulsive disorder and the 3' region of neuronal glutamate transporter gene SLC1A1". American Journal of Medical Genetics. Part B, Neuropsychiatric Genetics. 162B (4): 367–79. doi:10.1002/ajmg.b.32137. PMID 23606572.
^ Pooley, EC; Fineberg, N; Harrison, PJ (June 2007). "The met(158) allele of catechol-O-methyltransferase (COMT) is associated with obsessive-compulsive disorder in men: case-control study and meta-analysis". Molecular Psychiatry. 12 (6): 556–61. doi:10.1038/sj.mp.4001951. PMID 17264842.
^ Azzam, A; Mathews, CA (15 November 2003). "Meta-analysis of the association between the catecholamine-O-methyl-transferase gene and obsessive-compulsive disorder". American Journal of Medical Genetics. Part B, Neuropsychiatric Genetics. 123B (1): 64–9. doi:10.1002/ajmg.b.20013. PMID 14582147.
^ Bracha HS (2006). "Human brain evolution and the "Neuroevolutionary Time-depth Principle:" Implications for the Reclassification of fear-circuitry-related traits in DSM-V and for studying resilience to warzone-related posttraumatic stress disorder". Progress in Neuro-Psychopharmacology and Biological Psychiatry. 30 (5): 827–853. doi:10.1016/j.pnpbp.2006.01.008. PMID 16563589.
^ ab Boileau B (2011). "A review of obsessive-compulsive disorder in children and adolescents". Dialogues Clin Neurosci. 13 (4): 401–11. PMC 3263388. PMID 22275846.
^ Moretto, Germana; Pasquini, Massimo; et al. (2008), "What every psychiatrist should know about PANDAS: a review", Clinical Practice and Epidemiology in Mental HealthCS1 maint: Explicit use of et al. (link)
^ Pearlman, DM; Vora, HS; Marquis, BG; Najjar, S; Dudley, LA (July 2014). "Anti-basal ganglia antibodies in primary obsessive-compulsive disorder: systematic review and meta-analysis". The British Journal of Psychiatry. 205 (1): 8–16. doi:10.1192/bjp.bp.113.137018. PMID 24986387.
^ Rotge, Jean-Yves; Guehl, Dominique; Dilharreguy, Bixente; Cuny, Emmanuel; Tignol, Jean; Bioulac, Bernard; Allard, Michele; Burbaud, Pierre; Aouizerate, Bruno (3 March 2017). "Provocation of obsessive–compulsive symptoms: a quantitative voxel-based meta-analysis of functional neuroimaging studies". Journal of Psychiatry & Neuroscience : JPN. 33 (5): 405–412. ISSN 1180-4882. PMC 2527721. PMID 18787662.
^ Whiteside, Stephen P.; Port, John D.; Abramowitz, Jonathan S. (2004). "A meta–analysis of functional neuroimaging in obsessive–compulsive disorder". Psychiatry Research: Neuroimaging. 132 (1): 69–79. doi:10.1016/j.pscychresns.2004.07.001. PMID 15546704.
^ Rasgon, A; Lee, WH; Leibu, E; Laird, A; Glahn, D; Goodman, W; Frangou, S (October 2017). "Neural correlates of affective and non-affective cognition in obsessive compulsive disorder: A meta-analysis of functional imaging studies". European Psychiatry. 46: 25–32. doi:10.1016/j.eurpsy.2017.08.001. PMID 28992533.
^ Brem, Silvia; Grünblatt, Edna; Drechsler, Renate; Riederer, Peter; Walitza, Susanne (1 January 2014). "The neurobiological link between OCD and ADHD". Attention Deficit and Hyperactivity Disorders. 6 (3): 175–202. doi:10.1007/s12402-014-0146-x. ISSN 1866-6116. PMC 4148591. PMID 25017045.
^ Amerio, Andrea; Stubbs, Brendon; Odone, Anna; Tonna, Matteo; Marchesi, Carlo; Nassir Ghaemi, S. (17 August 2016). "Bipolar I and II Disorders; A Systematic Review and Meta-Analysis onDifferences in Comorbid Obsessive-Compulsive Disorder". Iranian Journal of Psychiatry and Behavioral Sciences. 10 (3): e3604. doi:10.17795/ijpbs-3604. ISSN 1735-8639. PMC 5098723. PMID 27826323.
^ Piras, Federica; Piras, Fabrizio; Chiapponi, Chiara; Girardi, Paolo; Caltagirone, Carlo; Spalletta, Gianfranco (1 January 2015). "Widespread structural brain changes in OCD: a systematic review of voxel-based morphometry studies". Cortex. 62: 89–108. doi:10.1016/j.cortex.2013.01.016. ISSN 1973-8102. PMID 23582297.
^ Radua J, Mataix-Cols D (November 2009). "Voxel-wise meta-analysis of grey matter changes in obsessive–compulsive disorder". British Journal of Psychiatry. 195 (5): 393–402. doi:10.1192/bjp.bp.108.055046. PMID 19880927.
^ ab Radua J, van den Heuvel OA, Surguladze S, Mataix-Cols D (5 July 2010). "Meta-analytical comparison of voxel-based morphometry studies in obsessive-compulsive disorder vs other anxiety disorders". Archives of General Psychiatry. 67 (7): 701–711. doi:10.1001/archgenpsychiatry.2010.70. PMID 20603451.
^ Radua, J; Grau, M; van den Heuvel, OA; Thiebaut de Schotten, M; Stein, DJ; Canales-Rodríguez, EJ; Catani, M; Mataix-Cols, D (June 2014). "Multimodal voxel-based meta-analysis of white matter abnormalities in obsessive-compulsive disorder". Neuropsychopharmacology. 39 (7): 1547–57. doi:10.1038/npp.2014.5. PMC 4023155. PMID 24407265.
^ Friedlander, L; Desrocher, M (January 2006). "Neuroimaging studies of obsessive-compulsive disorder in adults and children". Clinical Psychology Review. 26 (1): 32–49. doi:10.1016/j.cpr.2005.06.010. PMID 16242823.
^ Stern, ER; Taylor, SF (September 2014). "Cognitive neuroscience of obsessive-compulsive disorder". The Psychiatric Clinics of North America. 37 (3): 337–52. doi:10.1016/j.psc.2014.05.004. PMID 25150566.
^ ab Wood, J; Ahmari, SE (2015). "A Framework for Understanding the Emerging Role of Corticolimbic-Ventral Striatal Networks in OCD-Associated Repetitive Behaviors". Frontiers in Systems Neuroscience. 9: 171. doi:10.3389/fnsys.2015.00171. PMC 4681810. PMID 26733823.
^ Nakao, Tomohiro; Okada, Kayo; Kanba, Shigenobu (August 2014). "Neurobiological model of obsessive-compulsive disorder: Evidence from recent neuropsychological and neuroimaging findings". Psychiatry and Clinical Neurosciences. 68 (8): 587–605. doi:10.1111/pcn.12195. PMID 24762196.
^ Barahona-Corrêa, JB; Camacho, M; Castro-Rodrigues, P; Costa, R; Oliveira-Maia, AJ (2015). "From Thought to Action: How the Interplay Between Neuroscience and Phenomenology Changed Our Understanding of Obsessive-Compulsive Disorder". Frontiers in Psychology. 6: 1798. doi:10.3389/fpsyg.2015.01798. PMC 4655583. PMID 26635696.
^ Davis, Kenneth L (2002). Neuropsychopharmacology : the fifth generation of progress : an official publication of the American College of Neuropsychopharmacology (5th ed.). Philadelphia, Pa.: Lippincott Williams & Wilkins. pp. 1609–1610. ISBN 978-0-7817-2837-9.
^ Muller, Christian P; Jacobs, Barry L; A Dijk; A Klompmakers; D Denys (2009). "4.4 The Serotonergic System in Obsessive-Compulsive Disorder". Handbook of the behavioral neurobiology of serotonin (1st ed.). London: Academic. pp. 547–558. ISBN 978-0-12-374634-4.
^ Kim KW, Lee DY (2002). "Obsessive-Compulsive Disorder Associated With a Left Orbitofrontal Infarct". Journal of Neuropsychiatry and Clinical Neurosciences. 14 (1): 88–89. doi:10.1176/appi.neuropsych.14.1.88. PMID 11884667.
^ Wood, Jesse; Ahmari, Susanne E. (17 December 2015). "A Framework for Understanding the Emerging Role of Corticolimbic-Ventral Striatal Networks in OCD-Associated Repetitive Behaviors". Frontiers in Systems Neuroscience. 9. doi:10.3389/fnsys.2015.00171. ISSN 1662-5137. PMC 4681810. PMID 26733823.
^ ab Pittenger, Christopher; Bloch, Michael H.; Williams, Kyle (3 March 2017). "GLUTAMATE ABNORMALITIES IN OBSESSIVE COMPULSIVE DISORDER: NEUROBIOLOGY, PATHOPHYSIOLOGY, AND TREATMENT". Pharmacology & Therapeutics. 132 (3): 314–332. doi:10.1016/j.pharmthera.2011.09.006. ISSN 0163-7258. PMC 3205262. PMID 21963369.
^ Graat, I; Figee, M; Denys, D. "Neurotransmitter Dysregulation in OCD". In Pittinger, C. Obsessive-Compulsive Disorder: Phenomenology, Pathophysiology and Treatment. Oxford University Press.
^ Aoki, Y; Aoki, A; Suwa, H (14 August 2012). "Reduction of N-acetylaspartate in the medial prefrontal cortex correlated with symptom severity in obsessive-compulsive disorder: meta-analyses of (1)H-MRS studies". Translational Psychiatry. 2 (8): e153. doi:10.1038/tp.2012.78. PMC 3432192. PMID 22892718.
^ ab Quick Reference to the Diagnostic Criteria from DSM-IV-TR. Arlington, VA: American Psychiatric Association, 2000.
^ Starcevic, V; Janca, A (January 2011). "Obsessive-compulsive spectrum disorders: still in search of the concept-affirming boundaries". Current Opinion in Psychiatry. 24 (1): 55–60. doi:10.1097/yco.0b013e32833f3b58. PMID 20827198.
^ ab Aardema F., O'Connor (2007). "The menace within: obsessions and the self". International Journal of Cognitive Therapy. 21 (3): 182–197. doi:10.1891/088983907781494573.
^ Aardema F., O'Connor (2003). "Seeing white bears that are not there: Inference processes in obsessions". Journal of Cognitive Psychotherapy. 17: 23–37. doi:10.1891/jcop.17.1.23.58270.
^ ab Carter, K. "Obsessive–compulsive personality disorder." PSYC 210 lecture: Oxford College of Emory University. Oxford, GA. 11 April 2006.
^ ab National Institute for Health and Clinical Excellence (NICE) (November 2005). "Obsessive-compulsive disorder: Core interventions in the treatment of obsessive-compulsive disorder and body dysmorphic disorder". Information about NICE Clinical Guideline 31. UK National Health Service (NHS). Archived from the original on 12 January 2017. Retrieved 24 July 2016.
^ Koran LM, Hanna GL, Hollander E, Nestadt G, Simpson HB (July 2007). "Practice guideline for the treatment of patients with obsessive-compulsive disorder". The American Journal of Psychiatry. 164 (7 Suppl): 5–53. PMID 17849776.
^ ab Huppert & Roth: (2003) Treating Obsessive-Compulsive Disorder with Exposure and Response Prevention. The Behavior Analyst Today, 4 (1), 66 – 70 BAO Archived 23 March 2010 at the Wayback Machine.
^ Klein DF (2000). "Flawed meta-analyses comparing psychotherapy with pharmacotherapy". Am J Psychiatry. 157 (8): 1204–11. doi:10.1176/appi.ajp.157.8.1204. PMID 10910778.
^ Arroll B, Elley CR, Fishman T, Goodyear-Smith FA, Kenealy T, Blashki G, Kerse N, Macgillivray S (2009). Arroll, Bruce, ed. "Antidepressants versus placebo for depression in primary care". The Cochrane Database of Systematic Reviews (3): CD007954. doi:10.1002/14651858.CD007954. PMID 19588448.CS1 maint: Multiple names: authors list (link)
^ "Review Finds SSRIs Modestly Effective in Short-Term Treatment of OCD". Archived from the original on 13 April 2013.
^ Fineberg NA, Brown A, Reghunandanan S, Pampaloni I (2012). "Evidence-based pharmacotherapy of obsessive-compulsive disorder". The International Journal of Neuropsychopharmacology. 15 (8): 1173–91. doi:10.1017/S1461145711001829. PMID 22226028.
^ "Sertraline prescribing information" (PDF). Archived (PDF) from the original on 16 June 2015. Retrieved 30 January 2015.
^ "Paroxetine prescribing information" (PDF). Archived from the original (PDF) on 19 February 2015. Retrieved 30 January 2015.
^ Komossa, K; Depping, AM; Meyer, M; Kissling, W; Leucht, S (8 Dec 2010). "Second-generation antipsychotics for obsessive compulsive disorder". The Cochrane Database of Systematic Reviews (12): CD008141. doi:10.1002/14651858.CD008141.pub2. PMID 21154394.
^ Pignon, B; Tezenas du Montcel, C; Carton, L; Pelissolo, A (7 November 2017). "The Place of Antipsychotics in the Therapy of Anxiety Disorders and Obsessive-Compulsive Disorders". Current Psychiatry Reports. 19 (12): 103. doi:10.1007/s11920-017-0847-x. PMID 29110139.
^ Koran, Lorrin; Hanna, Gregory; Hollander, Eric; Nestadt, Gerald; Helen, Simpson. "Practice Guideline for the Treatment of Patients With Obsessive-Compulsive Disorder" (PDF). American Psychiatric Association. American Psychiatric Association.
^ Cybulska Eva M (2006). "Obsessive Compulsive disorder, the brain and electroconvulsive therapy". British Journal of Hospital Medicine. 67 (2): 77–82. doi:10.12968/hmed.2006.67.2.20466. PMID 16498907.
^ Barlow, D. H. and V. M. Durand. Essentials of Abnormal Psychology. California: Thomson Wadsworth, 2006.
^ Barlas S (8 April 2009). "FDA Approves Pioneering Treatment for Obsessive- Compulsive Disorder". Psychiatric Times. 26 (4). Archived from the original on 10 July 2009.
^ Surgical Procedures for Obsessive–Compulsive Disorder Archived 25 July 2008 at the Wayback Machine., by M. Jahn and M. Williams, Ph.D,. BrainPhysics OCD Resource, Accessed 6 July 2008.
^ O'Donohue William; Ferguson Kyle E (2006). "Evidence-Based Practice in Psychology and Behavior Analysis". The Behavior Analyst Today. 7 (3): 335–347. doi:10.1037/h0100155.
^ ab Freeman, J; Garcia, A; Frank, H; Benito, K; Conelea, C; Walther, M; Edmunds, J (2014). "Evidence base update for psychosocial treatments for pediatric obsessive-compulsive disorder". Journal of Clinical Child and Adolescent Psychology. 43 (1): 7–26. doi:10.1080/15374416.2013.804386. PMC 3815743. PMID 23746138.
^ Rapoport, J. E. (1989). Obsessive-compulsive Disorder In Children & Adolescents. Washington: American Psychiatric Press.
^ Adams, P. L. (1973). Obsessive Children: A Sociopsychiatric Study. Philadelphia: Brunner / Mazel.
^ D'Alessandro TM (2009). "Factors influencing the onset of childhood obsessive compulsive disorder". Pediatr Nurs. 35 (1): 43–6. PMID 19378573.
^ Chen YW, Dilsaver SC (1995). "Comorbidity for obsessive-compulsive disorder in bipolar and unipolar disorders". Psychiatry Research. 59 (1–2): 57–64. doi:10.1016/0165-1781(95)02752-1. PMID 8771221.
^ Angelakis, I; Gooding, P; Tarrier, N; Panagioti, M (July 2015). "Suicidality in obsessive compulsive disorder (OCD): a systematic review and meta-analysis". Clinical Psychology Review. 39: 1–15. doi:10.1016/j.cpr.2015.03.002. PMID 25875222.
^ Turner J, Drummond LM, Mukhopadhyay S, Ghodse H, White S, Pillay A, Fineberg NA (June 2007). "A prospective study of delayed sleep phase syndrome in patients with severe resistant obsessive–compulsive disorder". World Psychiatry. 6 (2): 108–111. PMC 2219909. PMID 18235868.
^ Paterson JL, Reynolds AC, Ferguson SA, Dawson D (2013). "Sleep and obsessive-compulsive disorder (OCD)". Sleep Medicine Reviews. 17 (6): 465–74. doi:10.1016/j.smrv.2012.12.002. PMID 23499210.
^ Mineka S, Watson D, Clark LA (1998). "Comorbidity of anxiety and unipolar mood disorders". Annual Review of Psychology. 49: 377–412. doi:10.1146/annurev.psych.49.1.377. PMID 9496627.
^ Pediatric Obsessive-Compulsive Disorder Differential Diagnoses Archived 17 September 2012 at the Wayback Machine. – 2012
^ Mansueto CS, Keuler DJ (2005). "Tic or compulsion?: it's Tourettic OCD". Behavior Modification. 29 (5): 784–99. doi:10.1177/0145445505279261. PMID 16046664.
^ "OCD and Tourette Syndrome: Re-examining the Relationship". International OCD Foundation. Archived from the original on 1 November 2013. Retrieved 30 October 2013.
^ Abramovitch Amitai, Anholt Gideon, Raveh-Gottfried Sagi, Hamo Naama, Abramowitz Jonathan S (2017). "Meta-Analysis of Intelligence Quotient (IQ) in Obsessive-Compulsive Disorder". Neuropsychology Review. 28 (1): 111–120. doi:10.1007/s11065-017-9358-0. PMID 28864868.CS1 maint: Multiple names: authors list (link)
^ Pallanti, S; Grassi, G; Sarrecchia, ED; Cantisani, A; Pellegrini, M (2011). "Obsessive-compulsive disorder comorbidity: clinical assessment and therapeutic implications". Frontiers in Psychiatry. 2: 70. doi:10.3389/fpsyt.2011.00070. PMC 3243905. PMID 22203806.
^ Eddy KT, Dutra L, Bradley R, Westen D (2004). "A multidimensional meta-analysis of psychotherapy and pharmacotherapy for obsessive-compulsive disorder". Clin Psychol Rev. 24 (8): 1011–30. doi:10.1016/j.cpr.2004.08.004. PMID 15533282.
^ Subramaniam, M; Soh, P; Vaingankar, JA; Picco, L; Chong, SA (May 2013). "Quality of life in obsessive-compulsive disorder: impact of the disorder and of treatment". CNS Drugs. 27 (5): 367–83. doi:10.1007/s40263-013-0056-z. PMID 23580175.
^ Boileau, B (2011). "A review of obsessive-compulsive disorder in children and adolescents". Dialogues in Clinical Neuroscience. 13 (4): 401–11. PMC 3263388. PMID 22275846.
^ abcdefghijklmnopqrstuvwxyzaa Osborn, Ian (1998). Tormenting Thoughts and Secret Rituals: The Hidden Epidemic of Obsessive-Compulsive Disorder. New York City, New York: Dell Publishing. ISBN 978-0-440-50847-2.
^ ab M. A. Jenike; Baer, L.; & W. E. Minichiello. Obsessive Compulsive Disorders: Theory and Management. Littleton, MA: PSG Publishing, 1986.
^ Berrios, G E (1989). "Obsessive Compulsive Disorder: Its conceptual history in France during the 19th Century". Comprehensive Psychiatry. 30 (4): 283–95. doi:10.1016/0010-440x(89)90052-7. PMID 2667880.
^ Freud S (1950). Totem and Taboo:Some Points of Agreement between the Mental Lives of Savages and Neurotics. trans. Strachey. New York: W. W. Norton & Company. ISBN 978-0-393-00143-3. p. 29.
^ "SAMUEL JOHNSON (1709–1784): A Patron Saint of OCD? by Fred Penzel, Ph.D. from the Scientific Advisory Board of the International OCD Foundation". Westsuffolkpsych.homestead.com. Archived from the original on 15 June 2013. Retrieved 29 November 2013.
^ Dittmann, M (July–August 2005). "Hughes's germ phobia revealed in psychological autopsy". American Psychological Association. Archived from the original on 5 January 2015. Retrieved 9 January 2015.
^ M. Dittmann (July–August 2005). "Hughes's germ phobia revealed in psychological autopsy". APA Online: Monitor on Psychology. 36 (7). Archived from the original on 29 December 2008.
^ Chosak, Anne (12 October 2012). "The Aviator: A real-life portrayal of OCD in the media". =Massachusetts General Hospital OCD and Related Disorders Program. Archived from the original on 22 February 2015. Retrieved 9 January 2015.
^ Goldberg FR (2007). Turn box office movies into mental health opportunities: A literature review and resource guide for clinicians and educators (PDF). Beneficial Film Guides, Inc. p. 8. Archived from the original (PDF) on 8 July 2011. Retrieved 17 February 2010.
^ ab Berman, Noah (5 October 2012). "Is This 'As Good as It Gets?': Popular Media's Representation of OCD". Massachusetts General Hospital OCD and Related Disorders Program. Archived from the original on 22 February 2015. Retrieved 9 January 2015.
^ Almeida. "Royal College of Psychiatrists, Discover Psychiatry, Minds on Film Blog, Matchstick Men". Royal College of Psychiatrists. Archived from the original on 22 February 2015. Retrieved 14 January 2015.
^ Stewart, Susan (16 September 2007). "Happy to Be Neurotic, at Least Once a Week". The New York Times. Archived from the original on 11 December 2008. Retrieved 8 December 2008.
^ Aniety Disorders Association of America. "WHAT IS OCD?". USA Network. Archived from the original on 17 December 2008. Retrieved 8 December 2008.
^ Camfield DA, Sarris J, Berk M (1 June 2011). "Nutraceuticals in the treatment of obsessive compulsive disorder (OCD): a review of mechanistic and clinical evidence". Progress in Neuro-psychopharmacology & Biological Psychiatry. 35 (4): 887–95. doi:10.1016/j.pnpbp.2011.02.011. PMID 21352883.
^ Lakhan SE, Vieira KF (2008). "Nutritional therapies for mental disorders". Nutr J. 7: 2. doi:10.1186/1475-2891-7-2. PMC 2248201. PMID 18208598.
^ Davidson J, Bjorgvinsson T (June 2003). "Current and potential pharmacological treatments for obsessive-compulsive disorder". Expert Opinion on Investigational Drugs. 12 (6): 993–1001. doi:10.1517/13543784.12.6.993. PMID 12783603.
^ Koran LM (2007). "Obsessive-Compulsive Disorder: An Update for the Clinician". Focus (5): 3.
^ Wu K, Hanna GL, Rosenberg DR, Arnold PD (2012). "The role of glutamate signaling in the pathogenesis and treatment of obsessive–compulsive disorder". Pharmacology Biochemistry and Behavior. 100 (4): 726–735. doi:10.1016/j.pbb.2011.10.007. PMC 3437220. PMID 22024159.
External links
| Classification | D
|
|---|---|
| External resources |
|
| Wikimedia Commons has media related to Obsessive–compulsive disorder. |
Obsessive–compulsive disorder at Curlie
- National Institute Of Mental Health
- American Psychiatric Association
- APA Division 12 treatment page for obsessive-compulsive disorder
Davis, Lennard J. (2008). Obsession: A History. University of Chicago Press. ISBN 978-0-226-13782-7.
Authority control |
|
|---|
Categories:
- Obsessive–compulsive disorder
- Habit and impulse disorders
- Magical thinking
- Neurotic, stress-related and somatoform disorders
- Ritual
- Psychiatric diagnosis
- Anxiety
(window.RLQ=window.RLQ||).push(function(){mw.config.set({"wgPageParseReport":{"limitreport":{"cputime":"2.000","walltime":"2.288","ppvisitednodes":{"value":10260,"limit":1000000},"ppgeneratednodes":{"value":0,"limit":1500000},"postexpandincludesize":{"value":447474,"limit":2097152},"templateargumentsize":{"value":4738,"limit":2097152},"expansiondepth":{"value":14,"limit":40},"expensivefunctioncount":{"value":12,"limit":500},"unstrip-depth":{"value":1,"limit":20},"unstrip-size":{"value":377937,"limit":5000000},"entityaccesscount":{"value":4,"limit":400},"timingprofile":["100.00% 1851.770 1 -total"," 59.28% 1097.725 1 Template:Reflist"," 35.23% 652.418 83 Template:Cite_journal"," 9.43% 174.609 18 Template:Cite_web"," 8.07% 149.387 2 Template:Infobox"," 6.45% 119.463 1 Template:Infobox_medical_condition_(new)"," 4.00% 73.979 2 Template:Citation_needed"," 3.73% 69.052 2 Template:Fix"," 3.39% 62.815 1 Template:Medical_resources"," 3.38% 62.577 12 Template:Cite_book"]},"scribunto":{"limitreport-timeusage":{"value":"1.079","limit":"10.000"},"limitreport-memusage":{"value":9506816,"limit":52428800}},"cachereport":{"origin":"mw1265","timestamp":"20190106161824","ttl":1900800,"transientcontent":false}}});mw.config.set({"wgBackendResponseTime":125,"wgHostname":"mw1331"});});


